
1999
LEWES
18th OCTOBER 1999
INVOLVING
BRIGHTON DRIVER BOB KETTLE
Extracted and adapted from the report by the Health and Safety Executive
PHOTOGRAPHER UNKNOWN
At about 19.15 on 18 October 1999, at Lewes in East Sussex, the 17.52 passenger train from Victoria to Hastings collided with a train of empty coaches at a combined speed of about 30 mph. There were four members of staff and about twelve passengers on the trains. No-one was hurt, although one person was treated for shock at the scene.
The collision took place at a crossover near the junction where the lines from Haywards Heath and Brighton to Lewes meet.
There is no record of any previous train accident in this area.
Both trains were electric multiple-units. The passenger train consisted of twelve carriages, and the empty train of eight carriages, of class 421 ‘Mark 1' slam-door rolling stock.
H.S.E. investigations have concluded that the collision and subsequent derailment of the passenger train was caused by the driver of the passenger train starting his train away from Lewes station and passing a signal at danger. This was a result of human error. Both the signalling and braking systems have been tested and no evidence of any malfunction has been found. The signal involved had not previously been passed at danger.
Both trains sustained some damage in the collision. The crashworthiness of the trains has been reviewed by the Health & Safety Laboratory.
Consideration has been given to the prosecution of individuals and companies involved in the accident. However, it is the view of the Inspectorate that there is insufficient evidence to provide a realistic prospect of a conviction.
The Train Protection and Warning System (T.P.W.S.) is due to be fitted across the network and to all trains by the end of 2003.
TPWS consists of equipment on the track and the trains which will apply the brakes automatically: if a train is travelling above a predetermined speed on the approach to a red signal; if a train passes a red signal; and at some other key locations where passing a signal results in a high risk of collision. The signal involved in this accident is one that is due to be fitted with TPWS and the accident would have been prevented if it had been.
H.S.E. is satisfied with the recommendations made by the railway industry’s Formal Inquiry into the accident, and by action taken by Connex Rail to address some staff management issues. Implementation of these actions will be monitored by HSE. Accordingly, we have no additional recommendations to make.
Work to reduce the number of trains passing signals at danger (SPADs) is continuing, following the report produced by HSE in September 1999 on the railway industry's management of SPADs. This work is the subject of separate reports which are being
made available to the public.
The incident
At approximately 19.15 on Monday 18 October 1999, a short distance east of Lewes station in East Sussex, a collision took place between the 17.52 passenger train from Victoria to Hastings (train 1F34) (referred to as the passenger train in the rest of this report) and a train of empty coaches which should have formed the 17.16 Victoria to Eastbourne and Seaford train (5F30) (hereafter referred to as the empty train).
Both trains were operated by Connex South Central. Each train had a driver and a guard, and there were about twelve passengers on the Hastings train. There were no injuries in the collision, although one person was treated for shock at the scene.
The signalman at Lewes, whose box is directly opposite the site of the collision, called the emergency services who arrived within ten minutes.
Evacuation of people from the passenger train took place immediately via the two rear carriages which were still in the platform. Two other trains were trapped in open country at signals outside Lewes station. Passengers on one of them were
detrained by the driver and walked to the station, and those on the other train were walked to a nearby level crossing and collected by a bus. These operations were completed by 22.00.
The Sussex Police declared the accident site a "scene of crime", allowing them to restrict access to it pending an investigation.
After evacuation was completed, the scene was taken over by the British Transport Police (BTP). Initial investigations were conducted by the BTP and HSE, following which the area was handed back to the railway authorities at 02.45 on Tuesday 19 October. Recovery operations began immediately and following repairs to the track and conductor rails and testing of the signalling, normal working was resumed at 14.10 on the same day.
The weather at the time of the accident was dry and clear.
The trains
Both the trains were electric multiple-units, formed of 4-car class 421 (4- CIG) units of "mark 1" rolling stock. The passenger train consisted of twelve carriages (units 1850, 1805 and 1739), and the empty train 8 carriages (units 1845 and 1738). These trains were built between 1964 and 1972 at British Rail's York works. They have slam doors and are not fitted with central door locking. All the units were fitted with the BR Automatic Warning System (AWS) and the Driver's Reminder Appliance (DRA).
AWS is a device which alerts drivers to the indications shown by signals, and which will apply the train brakes automatically if the driver does not respond to it on the approach to a signal at "caution" or "danger”.
The DRA consists of a button and warning light on the driver's console which the driver should use to isolate the traction power when the train is stopped at a red signal.
Following the accident, all the carriages of both trains were removed to the Connex depot at Brighton, where full testing of their AWS, DRA, and braking systems was carried out. No faults were found.
The site and signalling
Lewes station, which is roughly triangular in shape, stands immediately west of the junction where the double track lines from Haywards Heath and Brighton converge. East of Lewes a double track runs towards Newhaven, Seaford, Eastbourne and Hastings. Trains travelling from and to Haywards Heath and London use platforms 1 and 2, while platforms 3, 4 and 5 serve the line to Brighton. A crossover east of the junction enables trains from both directions to reverse.
The lines from London, via Haywards Heath, curve sharply to the left on a radius of 200 yards as they pass through platform 1.
The track is then straight from the junction, opposite the signal box, for some 22 yards before curving to the right at a radius of 460 yards. The crossover where the collision occurred is 110 yards east of the junction.
Signalling in the area is controlled from Lewes signal box, located on the south side of the line a short distance from the point of collision. It is an old building, but contains an entrance-exit panel controlling two and three aspect main colour light signals and
position light shunting signals, which dates from 1976. Track Circuit Block regulations apply throughout the area. Extensive testing after the accident failed to reveal any faults in the signalling installation and HSE is satisfied that it was in good working
order.
The signal involved in the accident, LW3, is a three aspect colour light mounted on a short post at the top of the ramp at the east end of platform 1. It comes into view as a train rounds the curve through the platform (where speed is restricted to 20 mph) at a distance of about 80 yards. It has not previously been passed at danger. The overlap beyond the signal, intended to provide a safety margin in cases where a train driver misjudges braking, is 110 yards, which is better than the standard for the line speed.
This overlap extends over the junction between the Brighton and Haywards Heath lines. Accordingly, signal LW1 (the preceding signal to LW3 for trains approaching from Haywards Heath) cannot be cleared to allow a train to enter the station unless the junction itself is clear.
All running lines in the area are electrified at 750 volts DC on the conductor rail system. The supply is controlled from Railtrack's electrical control room at Brighton.
The course of events
Earlier in the day there had been severe disruption to train services caused by an incident when a car drove onto the line at a
level crossing near Arundel, and caught fire. Consequently, trains were being turned short of their destinations in an attempt to restore the booked service. The 17.16 had run empty from Victoria to Lewes because no guard was available. While it was en route a decision was taken to reverse it at Lewes and send it empty to the depot at Brighton.
The passenger train had started from Gatwick Airport instead of Victoria because of this disruption, and was running about fifteen minutes late as it approached Lewes. Signal LW1 was at caution (yellow) on the approach to the station and as the train entered platform 1 the driver noted that the signal at the end of the platform, LW3, was at danger (red). He received and acknowledged a correct AWS indication for this signal. The train stopped with the front of the cab at the '12 car' stop marker, which is fixed to the signal post at the top of the ramp at the end of the platform.
The empty train had passed through Lewes about five minutes before. It ran slowly through platform 1 and, as it passed through, the platform staff confirmed with the driver that the train was to be reversed at Lewes. After passing through the station, the train came to a stop at a position clear of the crossover points, no. 77. The driver changed ends by walking through the train then, driving from the west end cab, began the journey back through the crossover onto the up line. For this manoeuvre, which is regularly done at Lewes during disruptions to the service and engineering works, position light signal 58 was cleared by the
signalman, who routed the empty train through platform 4 towards Brighton.
The passenger train stopped at platform 1 and about 30 passengers left the train. Since the train had started from Gatwick Airport rather than Victoria, it had many fewer passengers than usual, and only about a dozen people were still on board when it left Lewes. The train started, passing signal LW3 at red, and accelerated until it reached about 20 mph.
The signalman on duty in Lewes signal box, which is located almost opposite the junction between the Haywards Heath and Brighton lines, was alerted by the sound of the passenger train moving off. Realising that a collision was imminent, he immediately transmitted a "General Stop” message on the Cab Secure Radio (CSR) system. Evidence from the data logging equipment which is part of the CSR indicates that this message was transmitted only seven seconds after the train occupied track circuit AH, thus fouling the junction. This very rapid response is much to the signalman's credit.
The driver of the passenger train, travelling on the down line, saw the empty train approaching from the opposite direction but because of the curvature of the line he thought it was on the up line. It was only when his train got very close to it that he realised that the empty train was coming through the crossover. At the same time he received the "General Stop" message on the radio display in his cab, together with an audible warning, and immediately applied the emergency brake. However, his train was still travelling at about 15 mph when it collided sidelong with the rear of the first carriage of the empty train, which was probably moving at about 15mph in the opposite direction. Neither train was fitted with a data recorder.
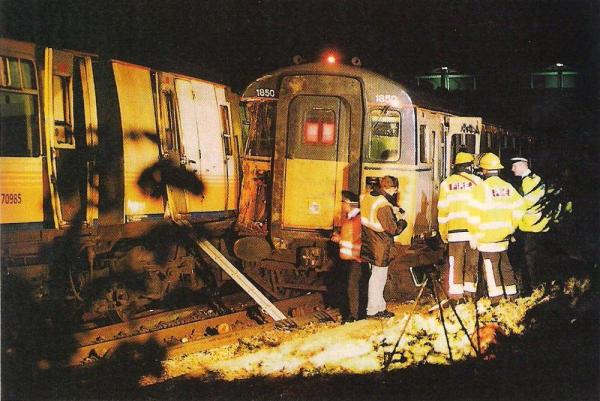
The leading bogie of the first carriage of the passenger train was derailed to the left and the right front corner of this carriage was badly damaged.
The empty train was not derailed. However, the first carriage suffered superficial damage to its rear end, while the second carriage was more severely damaged. The damage to the carriages and the crashworthiness of them is discussed in more detail below.

PHOTOGRAPHER UNKNOWN